Infectious Disease Response — to see the forest, not just the trees: What differentiated Japan from the Western countries?
Oshitani Hitoshi, Professor, Department of Virology, Tohoku University Graduate School of Medicine
―― COVID-19 (virus is SARS-CoV2) has spread globally and countries around the world are still working to suppress transmissions and treat patients.

Dr. Oshitani Hitoshi
Dr. Oshitani Hitoshi: The first report of COVID-19 by the Chinese government was at the end of last year, but it is likely that by late November, there were transmissions spreading in Wuhan City and surround areas of Hubei Province.
Spread of COVID-19 in Japan had two major waves so far. The first wave was originated by people with travel history to Wuhan and other places in China. From January to early February, the number of cases from China found in Japan was 11. Of course, there were considered to be more imported cases from China in reality, but it was likely somewhere around several tens to about a hundred. These people traveled to Japan for sightseeing or other purposes, and later, through places where people congregate, such as sports gyms and small concert houses, transmissions spread across the country including Hokkaido, Tokyo, Aichi, and Osaka. This first wave had come under control by mid March with number of cases relatively low, but the second wave came as the first wave was calming down.
Second wave was originated by infected people from a wide range of countries, such as Europe, US, Southeast Asia, and Egypt. We confirmed about 300 cases who had entered Japan from such countries, so the actual number of cases who entered Japan is estimated to be around 1,000 ~ 2,000. Although local transmissions of the second wave in Japan began in early February, infected people from abroad were coming to Japan and able to move around the country almost without any restriction, until the government put restrictions on travel at the end of March. This resulted in a large outbreak. The delay in action during that time is regrettable.
However, by early May, I believe that we managed to suppress the transmission of the second wave. At least, the second wave is already peaked. There will still be transmissions going forward, but we believe that we can maintain the number of new cases relatively low.
―― Do you think that the containment worked better than initially anticipated?
Dr. Oshitani: Once we understood the characteristics of this virus, we were confident that we could control the number of cases at a certain level. On the other hand, we had initially tried to keep the deaths below 100; however, we surpassed that. Now, we are continuing efforts to keep the number below 1,000.
Response measures differed among countries
―― Both domestic and overseas media have been critical of Japan’s response, saying that Japan has not conducted sufficient PCR testing, and thus do not have visibility into the full extent of the transmissions.
Dr. Oshitani: I do not believe that is true. At one point, Tokyo was often compared to New York City and some said it would to follow New York’s path. However, the first case was confirmed in New York City on March 1st. China had been detecting cases from last year, and Japan had already detected its first case on January 15th. Given that New York receives travelers from around the world, it is highly unlikely that there were no transmissions until March. It is more likely that they had overlooked “large scale transmissions” before March. That is probably the reason why New York is now facing a very challenging situation. If we had likewise overlooked cases in Tokyo, we would have been in the same situation as New York.
―― What differentiated Tokyo and New York?
Dr. Oshitani: Data clearly indicates that the measures taken by Japan have been more effective than those taken in Western countries. The difference was the strategy to suppress the transmission. In short, Japan’s strategy was “to see the forest to understand the whole”. Western countries, including New York City, focused more on seeing the trees instead.
Western countries thoroughly tested those who had come into contact with confirmed cases. By finding new cases, they focused on eliminating the virus one by one. However, data out of not only Japan but other countries have shown that positive rate among people who came into contact with cases are very low. On the other hand, transmissions can occur from mild and asymptomatic cases, which are difficult to find. Therefore, these measures were not very effective in containing the infection and led to a war of attrition.
The core of Japan’s strategy was not to overlook large sources of transmission. By accurately identifying what we call “clusters”, which are sources that have a potential to become a major outbreak, we were able to take measures for the surroundings of the clusters. By tolerating some degree of small transmissions, we avoided overexertion and nipped the bud of large transmissions. Behind this strategy is the fact that, for this specific virus, most people do not infect others, so even if we tolerate some cases go undetected, as long as we can prevent clusters where one infects many, most chains of transmissions will be dying out.
―― There are criticisms against Japan’s decision to limit testing.
Dr. Oshitani: From Western perspective, it may be unforgivable and unbearable to be in a limbo where you may have been infected but cannot be tested immediately. However, limiting access to testing and doctor visits was an important part of the response for this virus. Those who criticize this course of action do not see the forest for the trees.
Before we started counter-cluster measures in the cluster taskforce, Ministry of Health, Labour, and Welfare of Japan put forth a guideline on February 17th. According the guideline, those with mild symptoms should contact a Call Center for Japanese Returnees and Potential Contacts only when they have a fever of 37.5℃ or higher for four days . This policy of limiting testing was derived from experiences we had in the past with influenza outbreaks. When H1N1 influenza pandemic occurred in 2009, many people rushed to outpatient clinics to get tested. Not only did they have to wait many hours, the waiting areas became “3Cs” environments (3Cs refer to closed spaces, crowded places and close-contact settings.). That is why, at least among Japanese clinicians, there was a shared understanding that chaotic testing will actually make things worse.
In addition, there were issues of the quality of tests available. Especially in the US, PCR test kits of poor quality appeared because the US Food and Drug Administration (FDA) approved them prematurely. In addition, PCR primer (gene sequence) reported by China had low accuracy. Japan immediately stopped using it, but the US continued to use that primer. These factors combined lowered the overall accuracy and further fueled the confusion.
Transmission status: why were Western countries and Asia different?
―― Asia and western countries are having different experiences in transmissions. Situations are serious particularly in Europe and the U.S..
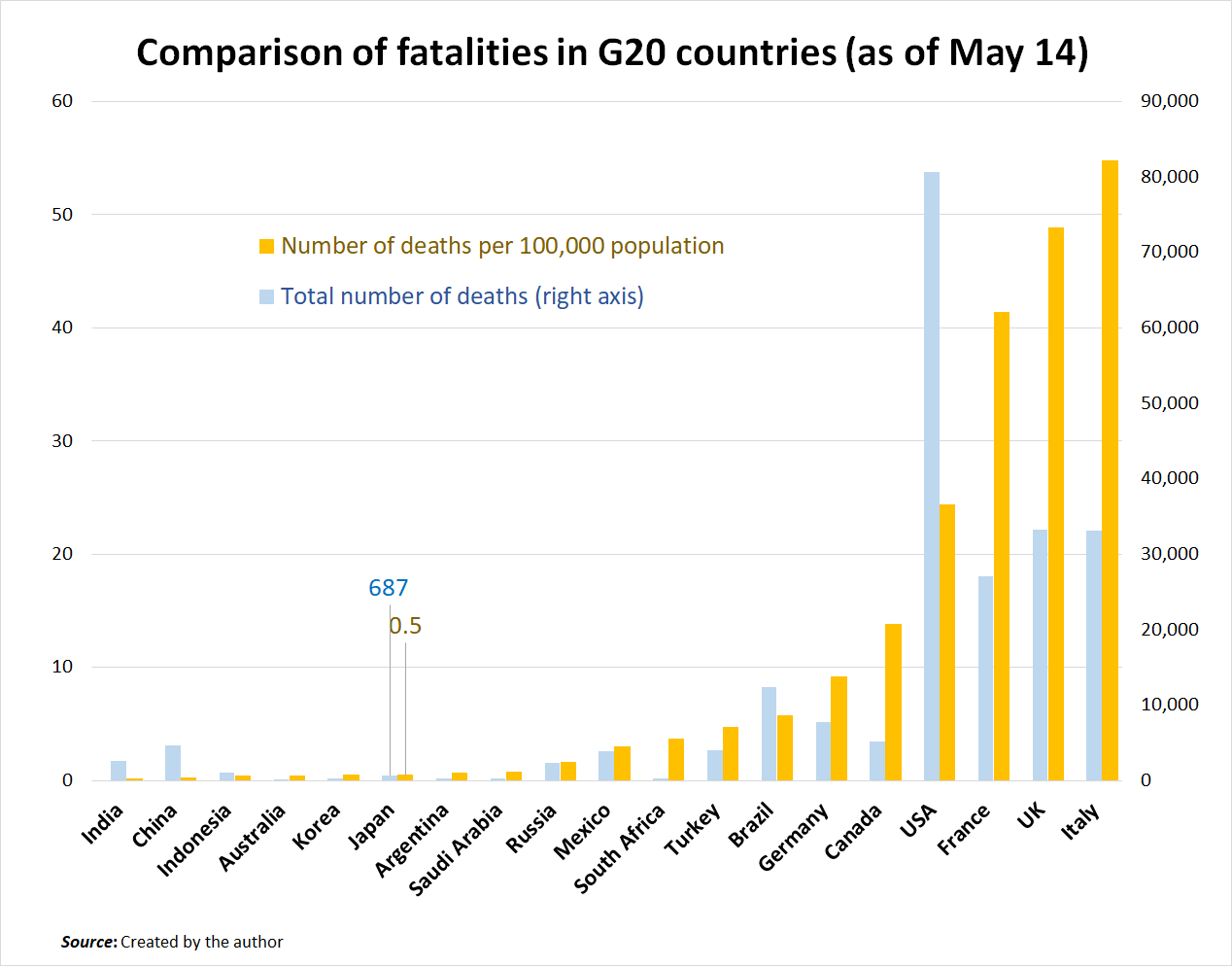
Dr. Oshitani: When you list the G20 countries by the number of deaths per 100,000, you can see that G7 countries other than Japan are all in very tough situations. (See the chart) Although increases in Brazil and Turkey are concerning, Asian and African countries are keeping both the numbers of confirmed cases and deaths relatively low in general. We do not know how the trends will continue going forward, but I feel that this is putting into question the ways of Western societies, that have led the world until today, as well as the ways how the entire world should be.
―― What factors do you think are at play?
Dr. Oshitani: I think that Western countries and Japan, or even Western countries and Asia, have fundamentally different ways of facing COVID-19, or even infectious diseases in general, including historical and cultural backgrounds.
I mentioned earlier that Western response was to identify cases and completely eliminate the virus. There is a notion of “completely annihilating the evil”. One way that is apparent is that not only politicians but even many academic experts have used war metaphors to talk about COVID-19.
On the other hand, it has been recorded in history that Japan has suffered through numerous outbreaks, such as smallpox, since Nara period (710 AD – 794 AD). Through that process, people have seen that there are powers beyond human understanding, and they accepted such powers to a certain extent. For example, there are shrines and temples across Japan that enshrine smallpox as “pox god”. Of course, it is an evil god, but it is recognized as a god. Also, a famous folk toy from Aizu region in Fukushima Prefecture called “akabeko (red cow)” has black dots on its body. There are theories that it represents smallpox. I guess Japan and other Asian societies have developed a relationship with infectious diseases that contains a sort of resignation, as we had accepted living together with microbes.

A famous folk toy from Aizu region in Fukushima Prefecture called “akabeko (red cow)”
Photo: Courtesy of Aizuwakamatsu City
Be ready for new threats in the post-COVID19 world
―― Going forward, are we going to be able to overcome COVID-19?
Dr. Oshitani: If that question is, “will Japan completely rid of COVID-19?”, then the answer is no. This is because it is impossible to detect all asymptomatic cases.
I personally believe that over the next year or several years, this virus will take root in our society. If we want to completely eradicate this virus, we need to run PCR testing on every single citizen of Japan for 2 weeks straight. This is not feasible, and there are still issues of accuracy of PCR tests due to their sensitivity.
―― There are people calling for herd immunity.
Dr. Oshitani: This is not an option. Herd immunity can be established if 70~80% of the population has immunity. Even in New York City where the situation is dire, if we trust the results of antibody testing, only 15~25% of people have been infected. To achieve over 70% of the population to have antibodies, New York City would need to repeat what they went through 3~4 times. Prime Minister Johnson of the UK also announced a policy towards herd immunity at one point, but took it back after a few days. Probably he realized that it was nonsense.
―― So what happens next?
Dr. Oshitani: In the short term, we, including Japan, cannot go back to the world before COVID-19. If we relax restrictions a little bit whenever transmissions decrease like the western countries are doing, it would increase transmissions again, and we would be fighting a war of attrition. Repeating that would destroy the economy and society.
So we need to change the way society works. We need to leverage telework more and need to rethink whether everyone needs to travel to Tokyo for work. Even if we change our behavior adapting to “a new lifestyle”, we need to be prepared for even the worst-case scenario in the long run.
I think that the next threat will be an influenza pandemic. The damage from 2009 pandemic was not too significant. A true pandemic in recent memory was the Hong Kong Flu of 1968, so it has already been over 50 years. A pandemic of an influenza virus for which no one has immunity could occur at any moment. And the infectivity of influenza is no match to that of COVID-19. If it happens in Japan, it will likely spread across the country within several weeks.
―― Could it be dealt with using a vaccine?
Dr. Oshitani: Even in the best-case scenario, production of vaccine will take several months. If clusters occur in the production facilities, production could halt. Even if we have stockpiles of the vaccines, it will still take several months to vaccinate all citizens, so it would not be fast enough to stop the transmissions. Other than the influenza virus, what if Ebola becomes airborne? What if bacteria that are resistant to all available drugs become widespread? Previous pandemic countermeasures will not work. It would not be surprising if the world 10 years from now takes infectious disease more seriously than climate change.
―― How would the global community need to respond?
Dr. Oshitani: The global community will also need to change in the post COVID-19 world. Based on experiences from COVID-19, we learned that a globalized world, in other words, an efficient world that prioritizes economic efficiency, is extremely vulnerable to infectious diseases. We are now being challenged whether we want to return to such a vulnerable world even after COVID-19.
―― Global collaboration around infectious diseases also need to be revisited.
Dr. Oshitani: Recently, people are becoming more interested in global health. However, we need to be questioning the old vertical structure where the rich help the poor – where the Western countries create guidelines that get implemented by lower-income countries. The WHO has been functioning as the intermediary between them.
However, it is suggestive that western countries, which have culture of trying to thoroughly eliminate threats of infectious diseases, all trapped themselves into dangerous situations, while Asian and African countries, which have adopted more of a “coexistence” approach, have been able to hold on up to this point. In addition, countries like Japan, China, South Korea, Taiwan, and Vietnam have all been successful with varying approaches. This indicates that the conventional vertical relationship and “one-size fits all” approach no longer make sense. We need to reconsider how international collaboration should be to respond to threats of infectious diseases with that understanding in mind. Japan has accumulated a wide range of knowhow through this experience. We believe that we can contribute to the world further by sharing our lessons.
Translated from “Kanto intabyu: Kansensho taisaku “Mori wo miru” shiko wo—Nani ga Nihon to Obei wo waketanoka (Infectious Disease Response – to see the forest, not just the trees: What differentiated Japan from the Western countries?),” Gaiko (Diplomacy), Vol. 61 May/Jun. 2020 pp. 6-11. (Courtesy of Toshi Shuppan) [June 2020]
Original article (Japanese):
http://www.gaiko-web.jp/test/wp-content/uploads/2020/06/Vol.61_6-11_Interview_New.pdf
Gaiko Vol. 61 (Japanese only): http://www.gaiko-web.jp/archives/2769
Keywords
- COVID-19
- coronavirus
- Japan’s response
- containment
- PCR testing
- New York
- clusters
- 3Cs
- new lifestyle
- vaccine
- herd immunity
- new threats
- influenza
- global collaboration
Related posts:
 Interview: Grand challenges posed to humanity by a viral disease
Interview: Grand challenges posed to humanity by a viral disease
 Between the “China Dream” and the “Pacific Alliance”: Japanese Strategy in an Age of US–China Rivalry
Between the “China Dream” and the “Pacific Alliance”: Japanese Strategy in an Age of US–China Rivalry
 Special Roundtable: Japanese Foreign Policy in 2020—Let us be a bond for a multilateral international order
Special Roundtable: Japanese Foreign Policy in 2020—Let us be a bond for a multilateral international order
 Trends in Selective Globalism
Trends in Selective Globalism
 The new Japonisme: From international cultural exchange to cultural diplomacy — Evaluating the influence of cultural activities on diplomacy
The new Japonisme: From international cultural exchange to cultural diplomacy — Evaluating the influence of cultural activities on diplomacy